GF COMMUNITY AND PUBLIC PRIVATE MIX (CPPM) GC7 PROJECT
Project year: 2024-2026
Location:Yamaltu Deba, Gombe State
Partners: LTR, SUFABEL, CHAD International


Project Overview
The burden of Tuberculosis (TB) remains a major public health challenge in Nigeria. To directly combat this crisis, Sufabel Community Development Initiatives (SCDI), serves as the Lead Community-Based Organization (CBO) for the implementation of the Global Fund CPPM Grant Cycle 7 (2024–2026) in Gombe State.
CHAD has been specifically engaged by SCDI to implement the critical Active Case Finding component of this project within Yamaltu Deba Local Government Area (LGA) of Gombe State.
Our partnership operates under the leadership of the Institute of Human Virology Nigeria (IHVN) and its Sub-Recipient, the Leprosy & Tuberculosis Relief Initiative Nigeria (LTR). This collaboration ensures that our community-level interventions are fully integrated into the National TB & Leprosy Control Programme (NTBLCP) strategy.
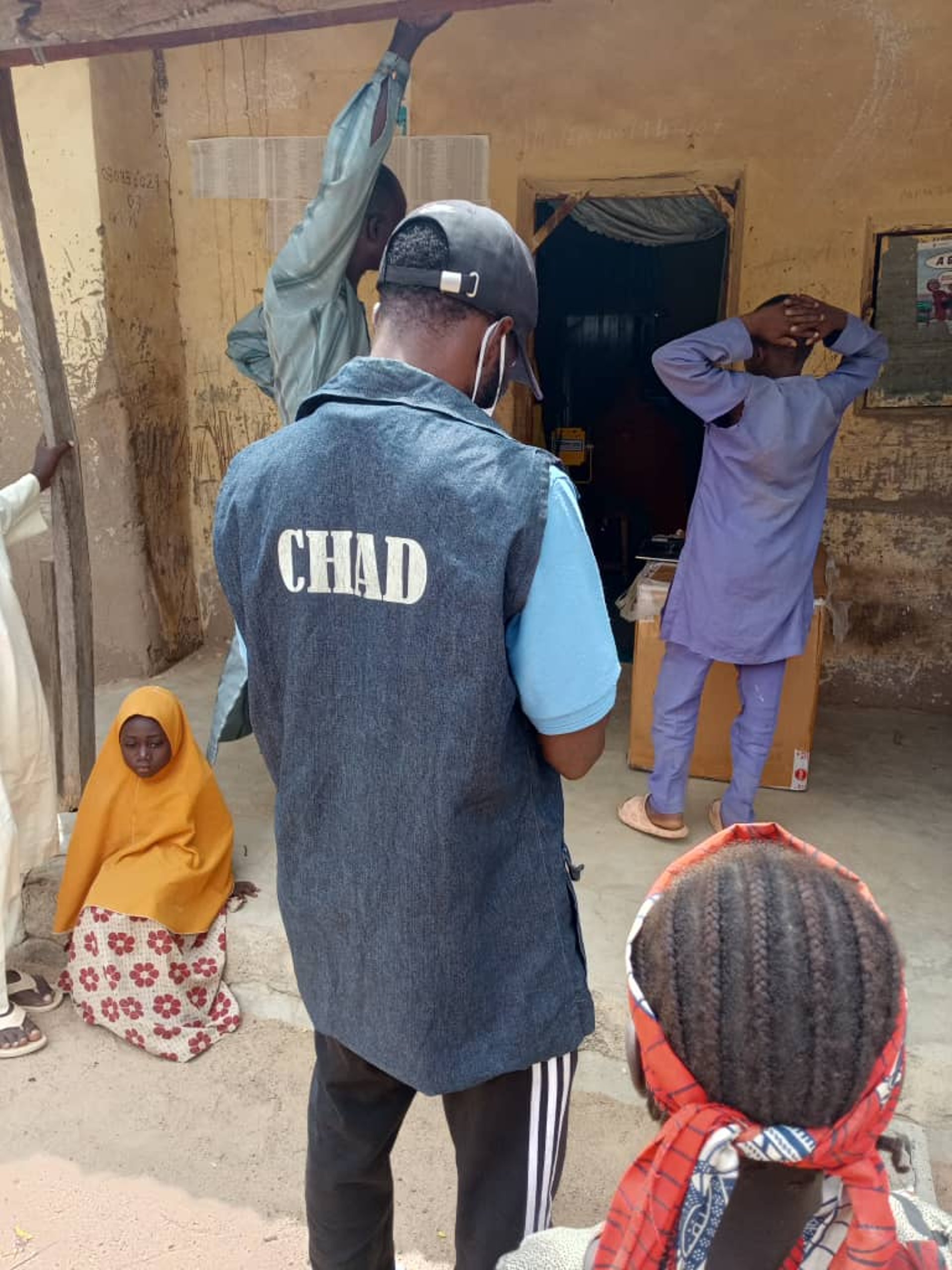
Field Action Pictures









Project Goal
The primary goal of this project is to Improve TB case finding, prevention, and link people with TB to treatment in DOTS centers across Yamaltu Deba LGA.
In essence, CHAD is dedicated to closing the "access gap," ensuring that no one in Yamaltu Deba is left behind due to geographical isolation, lack of information, or inadequate community tracking.

CHAD International: Closing the Tuberculosis Access Gap
Learn more about CHAD's community led strategy t endng t Tuberculosis in Gombe
As the Community-Based Organization (CBO) on the ground, CHAD is responsible for mobilizing the community and linking remote populations directly to clinical diagnosis and care. Our responsibilities ensure a comprehensive, end-to-end community intervention:
Conduct community-level mobilization, sensitization, and demand creation for TB services using Behaviour Change Communication (BCC) strategies.
Advocacy and Sensitization: Engage key community gatekeepers (traditional, religious, and government leaders) to build broad awareness and support for the initiative.
Case Finding: Actively participate in TB case finding activities, particularly targeting high-risk and remote populations.
Digital Screening: Utilize the ComTB App during daily activities to accurately screen individuals for TB symptoms and log all screenings for data accuracy.
Documentation & Accountability: Ensure all presumptive TB cases are accurately recorded in the DOTS Register, specifically marking the column "Referred by CV" to ensure accountability and track the vital contribution of community volunteers.
Sputum Collection: Collect sputum samples from all presumptive TB cases identified in the community.
Referral to Diagnosis: Conduct efficient sputum sample referrals to designated diagnostic sites.
Data Integrity: Update the DOTS Register with lab results and treatment statuses once available, ensuring a seamless data flow between the community and official health systems.
Volunteer Support: Provide effective supervision and monitoring of all community volunteers involved in the project, offering ongoing guidance and support to maintain high-quality data collection.
Official Liaison: Maintain monthly coordination with the Local Government TB & Leprosy Supervisor (LGTBLS) to cross-check registers and ensure complete data consistency with official health records.
Project Impact
CHAD's community-led Active Case Finding (ACF) strategy has been extremely successful in breaking down access and communication barriers, resulting in the direct identification and treatment of hundreds of individuals who would have otherwise remained untraced.
Since the project began, our teams have successfully screened a total of 4,200 individuals across the Yamaltu Deba LGA. This focused outreach led to the identification of 271 presumptive TB cases. Critically, our efficient logistics ensured that every single one of these presumptive cases all 271was successfully tested.
These efforts resulted in the diagnosis of 192 new drug-sensitive TB (DSTB) patients. These 192 individuals, who were previously hidden within the community and at risk of worsening illness, were immediately enrolled in treatment.
Impact Stories
Amina's Recovery
Amina represents the significant risk posed by undiagnosed TB within underserved communities. Her clinical presentation was consistently misinterpreted.
"The cough... the night sweats... it was constant. I was frequently diagnosed with asthma and ulcer at the facilities I visited," she reported. This prolonged misdiagnosis delayed effective treatment and maintained a risk of community transmission.
CHAD's Community - led strategy actively seeks out such hidden cases. Our community volunteers identified her, and diagnostic confirmation was swift. Amina was immediately linked to the appropriate DOTS treatment. Crucially, our system eliminated the logistical barrier: every dose of medication was personally delivered to her doorstep by our case worker.
Her recovery demonstrates that Active Case Finding is essential for correcting diagnostic delays and ensuring patients receive timely, targeted care.


Photo of Esther in her residence


Esther's Story
Esther's experience is a compelling case for the urgency of the TB project. She was presenting with severe, debilitating symptoms, indicating advanced disease progression.
"I had terrible headaches and coughing," she stated. Her subsequent comment leaves no doubt about the stakes: "When Umar came with the proper medicine... I believe if not for this intervention, I would have died."
This powerful testimony validates the necessity of CHAD's intervention model. By eliminating the time and distance required for patients to seek treatment, our team ensures that once a need is identified, the cure is delivered rapidly to the patient's home.
Esther is currently undergoing her full course of treatment and has shown significant improvement, achieving stability shortly after linkage. Her case demonstrates that CHAD’s caring bridge is an essential, life-saving mechanism that prevents fatal outcomes and ensures continuity of care throughout the lengthy treatment process.
Photo of Amina in her residence
Donor
Partners
PLAN International
CHAD International